Month: December 2014
ICD-10 Data: Why U.S. healthcare needs to move on from ICD-9 coding
by Carl Natale, ICD-10 Watch
When ICD-10 opponents say there is no benefit for patient care, they’re refusing to connect data to healthcare. It’s not hard to see why.
 It’s not like physicians can see a patient recover as their symptoms are documented. So there’s no clinical reason why U.S. healthcare needs more data.
It’s not like physicians can see a patient recover as their symptoms are documented. So there’s no clinical reason why U.S. healthcare needs more data.
Except data isn’t medicine. It doesn’t work that way. It accumulates over time to give healthcare professionals a picture of how treatments and diagnoses develop. That data can give physicians better ideas on how to treat their patients.
How much ICD-10 data do we need?
It’s hard to understand why U.S. healthcare needs data on turtle and jet engine injuries. Except someone with a medical degree argued for the inclusion of some “bizarre” codes. But those kinds of diagnosis codes are relatively few. There are more important specifics to focus on:
- Much of the specificity is due to laterality (right or left side).
- Also the new details included in the codes will help link symptoms and identify patients at risk of developing serious health problems.
- The precision allows for better tracking of care after the initial patient encounter. The information can be used to develop better care after treatment.
- Such specificity will help identify fraud, waste and abuse in medical claims. “Was the same procedure performed twice? Were conflicting claims filed for the same patient?”
And the better, more precise the data will help physicians make better decisions because they can see trends if they look at healthcare data.
How much time do we need for ICD-10 data to matter?
Again, the problem with this is that it’s going to take time to realize those benefits. Physicians and patients like short-term benefits. Take your medicine and you start to feel better in days or weeks. But it could take years to see these benefits.
All the knowledge that physicians use to diagnose and treat patients took years or decades or centuries to accumulate. Medicine is the result of careful study that takes time. And ICD-10 codes will help them accumulate data that leads to new treatments.
Will ICD-9 codes kill anyone?
Not likely. But medical uncertainty can. And it’s practically impossible to connect that with a lack of specificity in ICD-9 codes.
Just a little more specificity has got to help. And maybe ICD-10 codes can give us enough information about what we do not know that U.S. healthcare can advance treatment.
It’s a big maybe that comes at a cost for medical practices. But physicians deal a lot in maybes when they diagnose patients. Let’s use ICD-10 codes to get rid of a few maybes.
American Hospital Association sends letter to Congress supporting ICD-10 implementation date
On December 5, 2014, the American Hospital Association (AHA) issued a letter to Congressional leaders on behalf of its members imploring them to continue supporting the ICD-10 implementation date of October 1, 2015. Citing additional costs and disruptions of further delays along with the improved collaboration between the payer, provider, and government communities, the AHA is confident that the industry will be ready for the transitions which is now less than one year away.
CMS Releases Video Explaining ICD-10
No ICD-10 Delay included in recently passed Omnibus spending bill
Written by Chuck Buck, ICD-10 Monitor
Despite a significant lobbying effort mounted by a small but very vocal minority within the healthcare industry, the implementation of ICD-10 is expected to proceed without further delay.
The failed push marked a third attempt to delay the Oct. 1, 2015 ICD-10 implementation deadline well into 2017. Members of Congress rejected the request to include language that would again delay ICD-10 in the lame-duck omnibus spending bill that was passed by Congress on Dec. 11 and ratify by the Senate on Dec. 13.
Failing to delay ICD-10 by using a legislative maneuver – slipping language in a massive spending bill – represents a crippling blow to opposition that will make future efforts to revisit the matter very difficult. Congress made its decision not to hold up ICD-10 after hearing opinions about it from many voices in the healthcare community, including well-organized groups of physicians. During the course of this debate, there were many myths perpetuated, not to mention promises of doom and dysfunction, but also strong cases for proceeding with the coding system upgrade.
While fans of ICD-9 will no doubt use the March 2015 sustainable growth rate (SGR) bill to make another run at delaying implementation, it will be hard to convince members of Congress that more time is needed. If Congress didn’t see the need to enact a delay in December, why would they be convinced to delay months later in March?
Advocates for ICD-10, including the American Health Information Management Association (AHIMA), national and regional hospital associations, and physician groups are applauding the decision by Congress. Across the industry, companies and healthcare organizations have invested millions of dollars preparing for ICD-10. Many physicians have planned ahead for ICD-10 by taking advantage of low- and zero-cost education resources made available by the government.
Upon hearing the news that ICD-10 cleared a major legislative hurdle, organizations issued statements expressing their support for moving forward on this long-awaited and much-needed move to implement.
“Congress issued a strong message and sent the ‘delay ICD-10’ crowd back to the bench,” said Chris Powell, CEO of Precyse, a provider of health information management solutions and staunch advocate for ICD-10.
“I predict that, in a short time, the industry will look at the upsides of a modern coding system and wish that ICD-10 had arrived much sooner,” added Powell. “The vast majority of the industry is ready to move beyond ICD-9, an antiquated and very limited system that is woefully insufficient for hospitals, physicians, and patients. We have a myriad of best practices and learnings gained from other countries’ migrations to ICD-10 before us, and we now have the green light to put ICD-10 into motion.”
The impact of ICD-10 specificty on hospital operations
Edifecs, a healthcare technology company, recently conducted a survey of 454 industry representatives to identify what areas of hospital operations would most benefit from the increased specificty ICD-10. The chart below summarizes the opportunities.
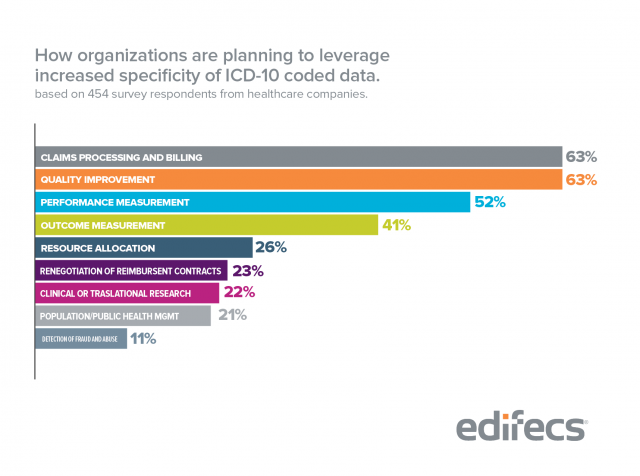
Given current reimbursement methodologies, these results are not surprising. However, as more ICD-10 claims data becomes available, it is reasonable to assume that the industry will strive to adjust coverage guidelines, medical necessity criteria, coding and billing requirements, and quality defintions.
ICD-10 is the Pathway to Big Data in Healthcare
by William Rusnak, MD
See full article here
If big data in healthcare is the future for medicine, then ICD-10 is the way to get there.
Forgetting the idea that this coding system is largely designed for better billing and that providers will eventually be forced to make the switch, let us take a look at the benefits of ICD-10.
Garbage in, garbage out
Although I’m well into my medicine career, I still think of myself as a struggling musician — a guy’s got to dream. Anyway, when recording in a studio, artists know all to well that when it comes to sound, poor-quality equipment will produce poor-quality audio, despite the development of truly impressive recording software. The same goes for medical data. The current coding system, ICD-9, is inflexible and far from comprehensive. “Garbage in” is a great way to describe it.
ICD-10 is an enormous expansion and at first glance seems excessive. Realistically, though, there is a finite amount of actions that a provider or patient can perform — or have happen to them. ICD-9 doesn’t even come close to meeting the descriptive needs of today’s environment. Alarmingly, there isn’t a code for Ebola. ICD-10, on the other hand, has 68,000 codes available for recording any diagnosis we can possibly imagine (plus ~72,000 more for procedures). Yes, it is comical and almost insane that some of the codes exist — see struck by a turtle and injured by a spacecraft — but that’s what being comprehensive is all about. Very often, physicians will conjure up the most unlikely, rare diagnoses for their differentials, but if they aren’t thinking about these “zebras”, they’ll never detect the one-in-a-million disease when it matters.
Ultimately, we are now in the world of “big data”, though very early in this new era. Our computing power is more than enough to adequately record human behavior in vital situations like receiving medical treatment and we need to capitalize on it. If a patient suffers the rarest of occurrences or undergoes an abstract procedure, there should be a code for it. Likewise, when a physician performs a specific procedure, a code should represent it in detail, including any variations. The first leap into big data is collecting it and that needs to be done with precision. Quality in, quality out.
We need to measure it to fix it
Some of the greatest success has been achieved by “going with the gut,” and often that is all a person can reply upon when making a decision. However, if there is a choice between proceeding blindly or having a team of scouts handing you an organized report detailing the outcomes of similar situations, most people will choose the latter. When decision-making is needed, life is simply better with data. If used properly, it can shed light upon complications within our systems that we otherwise would have overlooked. Google goes as far as saying that analyzing data will make us smarter, allowing us to anticipate problems before they occur.
As an example, look at nutrition. From my experience, when asked, many people will tell you that they “eat a pretty normal diet.” Now, make a decision with that data. Not very helpful, is it? Sure, a quick glance at the person can provide you with an answer like “it looks like it’s working,” but what advice can a physician or nutritionist possibly give without having the necessary details of the person’s diet? The same holds true for the rest of medical practice. Without measuring everything that we are doing in healthcare, improvement of our systems is going to be excessively difficult. A bird’s-eye view will be achieved when every medical organization in the country — eventually the world — is tracking events and outcomes with ICD-10. Only then will we have enough information to begin making the impactful changes needed to mend today’s broken system.
Public health, research, and quality improvement
As we finally move into this era of big data, consider the implications on public health and research. If our healthcare system is accurately collecting information about diseases and treatments in the form of codes, access to patient charts wouldn’t even be needed. The data would already be clean and organized, a scientist’s dream. Relationships between outcomes and treatments would quickly be revealed, allowing for optimization. Developing epidemics could be spotted significantly earlier. We will be able to learn in weeks what used to take years.
Last, data overload is a valid concern, but technology will help to “filter the noise” and facilitate the creation of plentiful, pertinent, organized, actionable data (not quite as catchy as “big data”, I know). Physicians will enjoy the luxury of practicing evidence-based medicine while the data unfolds in real-time. The old way of “keeping up with the literature” by reading medical journals each month will become extinct.
Big data is the future and for medicine, ICD-10 is the way to get there.
There’s a Code for That: W61.92
ICD-10 delay appears DOA in Congress this year
by Joseph Conn & Paul Demko
A proposal to delay implementation of ICD-10 diagnostic and procedure codes by an additional two years appears to be going nowhere in the current lame duck session of Congress.
“That’s not going to happen,” said a veteran healthcare consultant who tracks the issue closely, speaking on background. “The reports of them ever getting traction were overrated.”
The Texas Medical Association has been lobbying for the two-year delay. The nation’s largest state medical society for physicians, with 48,000 members, wants to push back the adoption date for the oft-delayed change to 2017.
The association’s position apparently found a champion in Rep. Pete Sessions (R-Texas), a nine-term incumbent who currently chairs the House Rules Committee. Sessions raised the possibility with House leadership of including such a provision in the budget agreement—what’s being billed the “cromnibus”—to keep the government funded, according to sources familiar with the discussions. Sessions’ office didn’t respond to a request for comment about the issue.
The federal government is set to run out of money Dec. 11 if Congress doesn’t authorize additional spending, making a funding bill a perfect vehicle for attaching special causes such as an ICD-10 delay since the overall bill must pass to keep the government open.
But the proposed ICD-10 delay, which would infuriate other interested healthcare parties that have been moving forward with plans to implement the coding changes next year, doesn’t appear to be going anywhere.
“(Sessions) definitely did make a play for it,” said the consultant, who has spoken with staffers in the offices of both the Republican and Democratic leadership. But “we are being told it is not going to happen.”
Coalition for ICD-10 Responds to AMA President Dr. Robert Wah
In his recent speech to the AMA House of Delegates, AMA president Dr. Robert Wah characterized the planned implementation of ICD-10 as analogous to the dark forces controlling the galaxy in the movie Star Wars:
“If it was a droid, ICD-10 would serve Darth Vader… For more than a decade, the AMA kept ICD-10 at bay – and we want to freeze it in carbonite!”
Dr. Wah’s attempt at humor is unfortunate because the quality and precision of our national health care data is a serious matter. In this country, we use coded data to assess quality of care, make benefit coverage decisions and to determine physician and hospital payment. The financial viability and performance assessments of hospitals and physicians are impacted by the data. Yet we continue to rely on an outdated 1970s-era coding system for reporting diagnoses and inpatient hospital procedures.
In his speech, Dr. Wah goes on to lament:
“Sucked into a jet engine? Burned by flaming water skis? Yes, there are codes for that.”
While at first glance these examples appear humorous, it is important to understand that these cause of injury codes were included in ICD-10 to meet the needs of organizations like the Department of Defense (aircraft accidents are an important issue for the military) and Worker’s Compensation (in waterski shows the burning waterski trick can lead to a worker’s comp claim). Should our national coding system ignore the needs of the Department of Defense and Worker’s Compensation?
Using cause of injury codes to imply that the coding detail in ICD-10 will be a burden to physicians is at best disingenuous because physicians are not required to report cause of injury codes, except in very limited situations such as injuries caused by medical treatment, like removing the wrong limb. Furthermore, the current ICD-9 system has similar cause of injury codes and their existence has never been a burden.
Dr. Wah continues to criticize by stating:
“We’d see 13,000 diagnosis codes balloon into 68,000 – a five-fold increase.”
Again, the inference is the increase is unnecessary and will be a burden for physicians. This is like saying the English language is a burden to use because there are 470,000 words in Webster’s unabridged English dictionary. Just as no one is expected to know rarely used words like floccinaucinihilipilification or use all 470,000 words, physicians and other providers will only use the codes relevant to their patient population (e.g., an ophthalmologist will primarily use only the eye codes).
The notion that more codes create a burden is out of touch with today’s digital world. As with almost everything else, there’s an app for that. In fact, there are more than 50 ICD-10 iPhone apps that allow a person to use word search to find an ICD-10 code instantaneously. Ranging from $1.99 to $10.99, the cost isn’t a burden (there are even a few free versions).
Dr. Wah complains about the number of codes and the detail in ICD-10 but fails to mention that much of the additional specificity in ICD-10 was at the request of medical specialty societies. Nor does he mention that there are no ICD-9 codes for many critical healthcare issues. There is no code to report and track Ebola. There are inadequate codes for tracking service-related health problems for our veterans. There are no codes to help us research sports-related concussions among young athletes. It’s hard to understand why the AMA is not demanding that this kind of information be available in our national data.
Dr. Wah goes on to state:
“We all know ICD-10 is expensive to implement. We don’t know if it will improve care.”
While there are significant costs associated with the implementation of ICD-10, the vast majority of the health care industry has already incurred those costs. In our digital world, the infrastructure for a systems change like ICD-10 has to be built and tested well in advance. These are sunk costs which will be lost if ICD-10 is not implemented. Indeed, CMS has estimated that the health care industry has already invested billions in preparation for ICD-10: “Forgoing ICD-10 translates into a loss of up to $22 billion for the U.S. health care industry” (Federal Register, 77(172), p 54689).
As to whether ICD-10 will improve care, it would seem obvious that more precise data should lead to better identification of potential quality problems and assessment of provider performance. There are multiple provisions in current law that alter Medicare payments for providers with excess patient complications. Unfortunately, the ICD-9 codes available to identify complications are woefully inadequate. If a patient experiences a complication from a graft or device, there is no way to specify the type of graft or device nor the kind of problem that occurred. How can we as a nation assess hospital outcomes, pay fairly, ensure accurate performance reports, and embrace value-based care if our coded data doesn’t provide such basic information? Doesn’t the public have a right to know this kind of information?
Our national healthcare data is broken due to the use of an archaic coding system. Given Dr. Wah’s “freeze it in carbonite” comment, it is clear that he is not really interested in a delay of ICD-10 but instead wants ICD-10 to never be implemented. It is hard to fathom why anyone would promote having our national data fail to meet the demands of 21st century health care. This is especially perplexing given that ICD-10 has been adopted by virtually every other country.
In attempting to relegate ICD-10 to the equivalent of “a galaxy far, far away,” Dr. Wah inexplicably ignores the implications for U.S. health care if we continue to use ICD-9 codes. This isn’t about waging a mythic battle (with sound bites instead of light-sabers). It’s about improving quality of care and patient safety in the here and now. It’s about ensuring fair payment, and in the case of Ebola, it’s about protecting our citizens. Yoda from Star Wars said it best: “Always in motion is the future…a little more knowledge lights our way.”